“Hysterectomy was the only option my doctor gave me.”
As a physician who has spent my career treating uterine fibroids without surgery and increasing fibroid awareness across the nation, I hear this sentence far too often.
The stories are always similar—that hysterectomy, or the surgical removal of the uterus, is the only treatment offered. Most of these women are unfamiliar with uterine fibroid embolization (UFE), a safe, outpatient, nonsurgical alternative. Almost all of the women telling me these experiences are African American.
Allow me to introduce myself. My name is John Lipman, MD, and I am a board certified interventional radiologist, renowned fibroid expert, and UFE specialist.

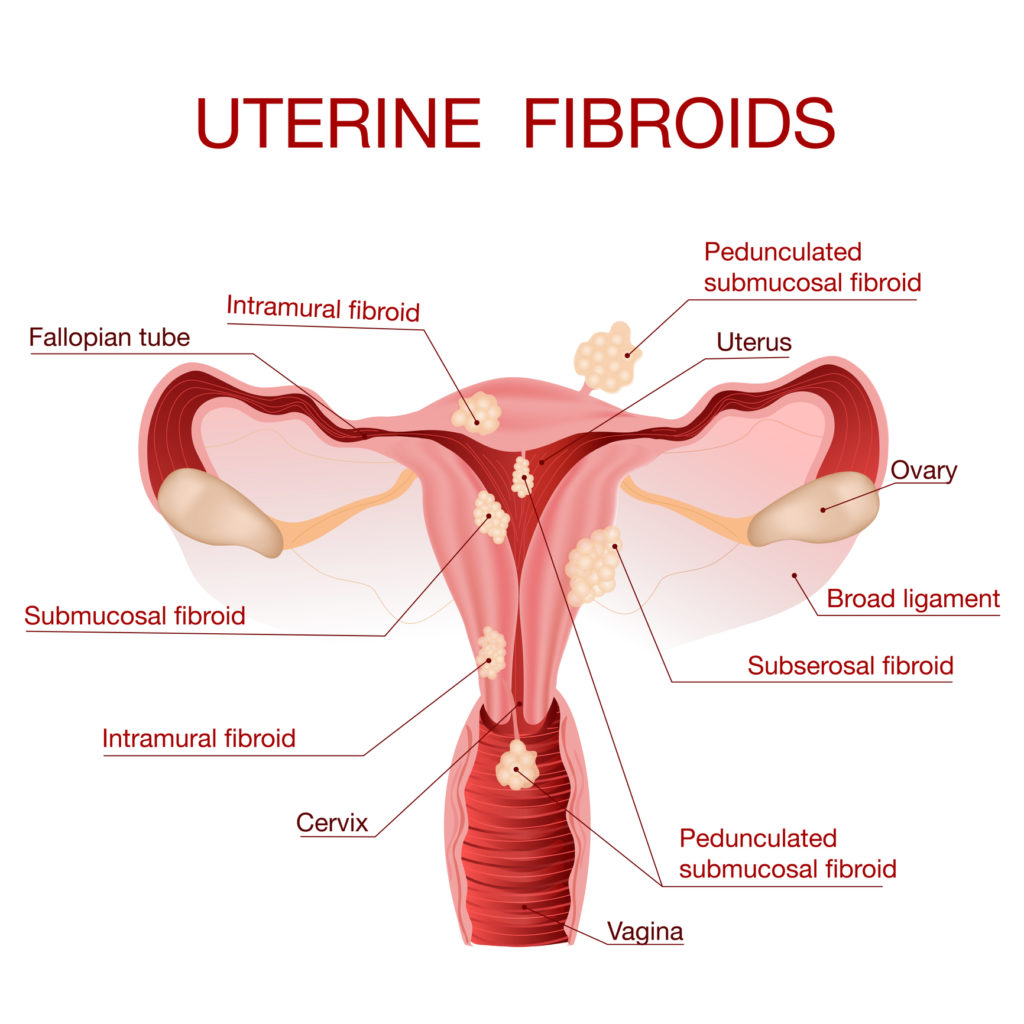
An estimated 11 million women1 in the U.S. are diagnosed with fibroids (noncancerous tumors in the uterine wall) and consequently many experience debilitating symptoms. These include heavy menstrual bleeding, pelvic pain and pressure, increased urinary frequency and waking up at night to urinate (nocturia), painful sex, and in some cases infertility. Eighty percent2 are women of color.
Research has shown that while Caucasian women undergo hysterectomy for uterine cancer (entirely appropriate), African American women are more likely to undergo hysterectomy for benign fibroids.3
Hysterectomy is a fibroid treatment option—but should be one of last resort. Hundreds of thousands of hysterectomies are done each year in the United States and the number one reason is fibroids.
The average age of a woman undergoing hysterectomy is





