
Imagine if what you thought were common features of aging were actually signs and symptoms of a life-threatening disease? That’s what happened to Randy. Randy, a 75-year-old man originally from Trinidad and Tobago, now living in New Orleans, was diagnosed with a hereditary form of transthyretin amyloid cardiomyopathy (ATTR-CM). ATTR-CM is a rare but life-threatening condition that is associated with heart failure.1,2 While he reached a diagnosis in 2018, the start of his symptoms date back to 2004.
As a retired professor of Modern Languages, Randy’s initial symptom of carpal tunnel syndrome seemed to be linked to his profession as he was connected to a keyboard for a majority of the workday. However, he began to notice tingling in his extremities, lack of stamina during his routine jogs, and shortness of breath. To Randy – and to many others with his condition – these symptoms were seemingly unrelated. Eventually, as his symptoms progressed, Randy realized that something was amiss, prompting him to continue following up with his doctor.
At first glance, Randy’s doctor attributed his shortness of breath to chronic obstructive pulmonary disease brought on by heavy smoking during his youth as well as the poor air quality in New Orleans. While this diagnosis may have been an explanation for Randy’s breathing problems, the other symptoms he was experiencing didn’t quite add up. Struggling to reach a proper diagnosis, Randy became increasingly frustrated and uncertain as to what was causing his health to deteriorate.
One day while climbing the stairs at his daughter’s townhouse, Randy was visibly having a lot of difficulty. By taking one look at him, his daughter knew he was in distress and rushed Randy to the ER. After receiving multiple diagnostic tests, he learned that he had congestive heart failure and the walls of his heart were stiff. Most ATTR-CM patients are diagnosed through a number of tests, including cardiac biopsy or nuclear scintigraphy (in addition to blood and urine tests). As part of Randy’s diagnostic testing, his cardiologist also gave him a genetic test, which helped inform his diagnosis of hereditary ATTR-CM.


“I was going to my primary care doctor about my shortness of breath, but the connection to ATTR-CM was not made. Once I got the diagnosis, my cardiologist was the main source of information but even so, I did a lot of research on my own. We really had to inform ourselves,” Randy recalled.
Unfortunately, Randy’s long road to diagnosis and difficulty finding information is an all too common experience for those with ATTR-CM. Awareness of the condition is low, even among primary care physicians and cardiologists, and as a result, it continues to be significantly underdiagnosed.3 For this reason, people with heart failure and their caregivers must advocate for themselves and discuss their symptoms with their cardiologists, who can run tests to confirm if they have the disease if the symptoms of ATTR-CM sound familiar.
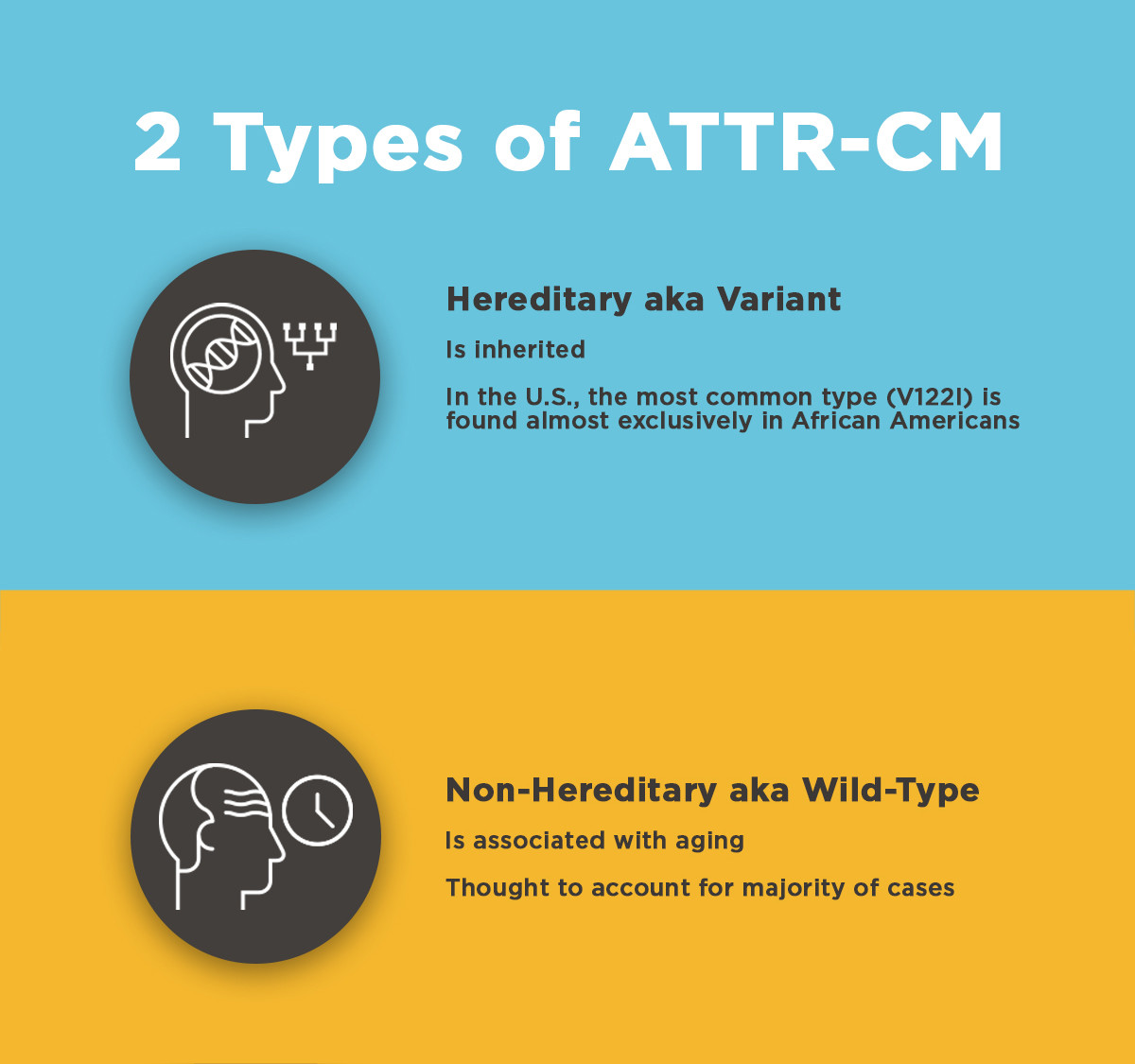
With the disproportionate rates of heart failure, heart attacks, and other serious heart conditions in the African-American community, it’s important to fully explore the underlying cause of these conditions with the help of a cardiologist.4,5 Attempting to find the underlying cause of your symptoms is especially important in the case of ATTR-CM. There are two forms of condition, hereditary or variant (hATTR) and wild-type (wtATTR). In the United States, the most common mutation associated with hereditary ATTR-CM, known as V122I (valine-to-isoleucine substitution at position 122), is found almost exclusively in people of African American, African or Afro-Caribbean descent.7,8 “The African-American community needs to be made aware of ATTR-CM. There needs to be a lot more done in order to publicize the symptoms of this disease, so more people can be aware and tested early,” Randy said.

It is important to clinically differentiate between ATTR and immunoglobulin light chain amyloidosis (AL), as they have different clinical courses, and AL requires immediate treatment.9 Once ATTR-CM is suspected, a cardiologist can perform several tests to help diagnose or identify risk of developing the disease, such as a non-invasive imaging test, called nuclear scintigraphy, and/or a cardiac biopsy. If a diagnosis of ATTR-CM is made, genetic testing and counseling may be suggested to confirm or rule out the hereditary form of ATTR-CM. Genetic testing is especially important in the African Americans who’ve been diagnosed with ATTR-CM, as it can help inform family members if they might be at risk for developing the condition.
You May Also Like

If you or a loved one have heart failure and are experiencing symptoms similar to Randy or other symptoms related to ATTR-CM, talk to your cardiologist and head over to www.YourHeartsMessage.com to learn more about this rare and life-threatening disease.
1 Ruberg FL, Berk JL. Transthyretin (TTR) cardiac amyloidosis. Circulation. 2012;126(10):1286-1300.
2 Rapezzi C, Quarta CC, Riva L, et al. Transthyretin-related amyloidoses and the heart: a clinical overview. Nat Rev Cardiol. 2010;7:398-408.
3 Rapezzi C, Lorenzini M, Longhi S, et al. Cardiac amyloidosis: the great pretender. Heart Fail Rev. 2015;20(2):117-124.
4 Graham G. Disparities in cardiovascular disease risk in the United States. Curr Cardiol Rev. 2015;11(3):238-245. doi:10.2174/1573403X11666141122220003.
5 Bonow RO, Grant AO, Jacobs AK. The cardiovascular state of the union: confronting healthcare disparities. Circulation. 2005;111(10):1205-1207.
6 Benson MD, Buxbaum JN, Eisenberg DS, et al. Amyloid nomenclature 2018: recommendations by the International Society of Amyloidosis (ISA) nomenclature committee. Amyloid. 2018;25(4):215-219.
7 Maurer MS, Hanna M, Grogan M, et al. Genotype and phenotype of transthyretin cardiac amyloidosis: THAOS (Transthyretin Amyloid Outcome Survey). J Am Coll Cardiol. 2016;68(2):161-172.
8 Jacobson DR, Alexander AA, Tagoe C, Buxbaum JN. Prevalence of the amyloidogenic transthyretin (TTR) V122I allele in 14 333 African-Americans. Amyloid. 2015;22(3):171-174.
9 Sperry BW, Ikram A, Hachamovitch R, et al. Efficacy of Chemotherapy for Light-Chain Amyloidosis in Patients Presenting With Symptomatic Heart Failure. J Am Coll Cardiol. 2016;67:2941-2948.